

Cone-Beam 3D and treatment plans: new decision-making paths
Authors: Daniele Benedetti Forastieri and Daniele Godi
It is now possible to introduce profound changes in case-specific difficulty/risk assessment processes by learning how to read three-dimensional (3D) data.
After decades-long use of two-dimensional (2D) exams, it may be that an intraoral X-ray exam or, even worse, an OPT, results in an instinctive initial diagnosis: a "fast" one, the speed of which actually seems to outweigh its objectivity.
However, subsequent assessment of the same case with 3D data can lead to a change in diagnosis and, therefore, in treatment, as it involves a thinking process that is "slow" because it requires analysis of a greater amount of data that is less familiar to us.
With training and experience, that "slow" process gradually becomes "fast" because the value of the 2D exam is diminished by the new 3D data assessment systems.
And we then find ourselves engaging in "fast" thinking processes based on data that our cognitive system previously needed time to take in.
Let us examine a case involving a complete upper arch rehabilitation plan based on 8 one-day implants, developed using the Cone-Beam 3D NewTom GiANO HR Professional.
The book "Thinking, Fast and Slow", published in 2012 and written by a psychologist Daniel Kahneman (also winner of the 2002 Nobel Prize in Economics), clearly explains the two fundamental “systems” the human mind employs during a decision-making processes.
On the one hand we have fast thinking, thoughts that are immediate and intuitive.
On the other there is slow thinking, that is, logic, involving thought-out decisions.
Kahneman draws up a comprehensive map of how thought is structured and the ways it works. He then goes on to suggest how we can oppose the "fast" mental mechanisms that are more likely to lead us astray and, instead, stimulate the "slow" ones that help us reason.
Introduction
Such an innovative technology undoubtedly generates a sense of wonder at first sight. More importantly, for at least 10 years now, technology has allowed dentists to drastically alter their approach to a variety of cases that involve operational risks and require a perfect comprehension of anatomically complex areas.
Understanding the rationale that lies behind the machine offers undisputed advantages.
I spoke with one of the four people who helped develop initial tomography technology into cone beam tomography.
The co-author of this article said: “As a trainer I've helped hundreds of dentists convert from 2D diagnostics to 3D diagnostics, and the biggest hurdle was never the software or the complexity of the device but, rather, the need to forget one diagnostic viewpoint and learn another".
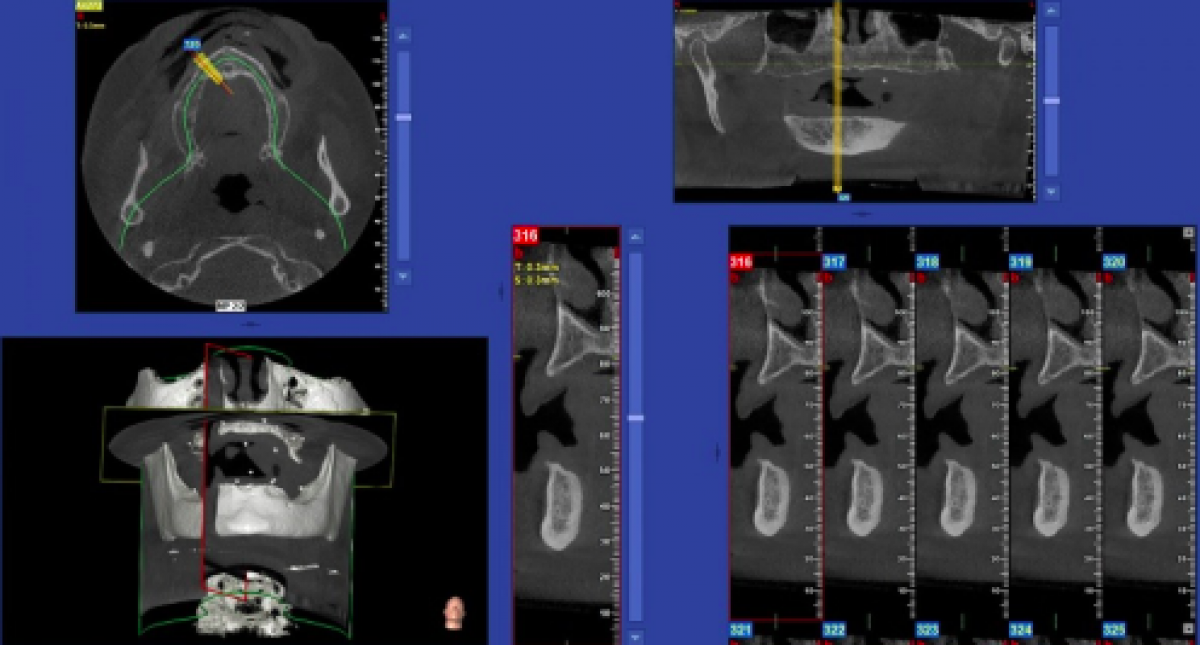
The first step of this process consists of assessing the anatomy - which training and tradition make us perceive as 2D - in its true three dimensions with the aid of 3D renderings (fig. 1-3) that enable us to locate cross-sections within the volume generated by the software (fig. 4, 5). Such 'slices' are, in fact, the tool of choice for exploring the acquired volume and making accurate, reliable measurements”.

Fig. 1 3D rendering, frontal

Fig. 2 3D rendering, patient's right side

Fig. 3 3D rendering, patient's left side

Fig. 4 Multiplanar image with details of ridge areas 11 and 12

Fig. 5 Multiplanar image with details of ridge areas 21 and 22
This conceptual "leap" has provided dentists with clear easy-to-interpret images. Moreover, these advanced systems can be installed directly in surgical offices and used in certain patients, in compliance with the standards and simple, clear guidelines.
However, the main topic of this paper concerns the interpretation of the examination and how it changes the analytical mechanisms we are - almost unconsciously - developing with regard to situations previously observed from a different perspective.
The first, necessary step that derives from the availability of Cone Beam data is to assess an individual (who "exists" in our minds in 2 dimensions, a perception nearly always attributable to academic training) in his/her true 3 dimensions.
No tool provides us with this viewpoint as effectively as volume that we can cross-section at will, preferably after mastering the rendering.
However, one must be fully aware that a rendering is not a dataset on which measurements should be made: those, in fact, must only be calculated on multiplanar reconstructions.
My experience in this field has profoundly changed my approach to the vast majority of cases I assess; moreover, the process of understanding and using this data has resulted in the difficulty 'bar' being gradually raised, again and again.
Moreover, this upward shift in limits is not followed by a reduction in the final risk coefficient. Remember: operations that were previously unimaginable are now within the realms of the possible. Therefore, the bar has also been raised on the risk front and such operations make post-op progress smoother improving post-healing quality of life.
There is another important aspect: this technology means we can treat more patients.
General principles to be observed when deciding whether or not to make a 3D exam
• ALARA (As Low As Reasonably Achievable) principle.
• Justification principle.
• Optimisation principle.
If the machine is your own, it is necessary to comply with the radiation protection regulations stated in the Council Directive 2013/59/Euratom of 5 December 2013, which contains three "recommendations" concerning individual examinations stating that they must be:
• contextual;
• integrated;
• non-postponable.
Tackling surgically complex - and also endodontic or orthodontic - cases by assessing 3D instead of 2D images lets a practitioner identify subtle pitfalls with "pre-operative awareness". Such situations may otherwise only be evident as the treatment progresses, and perhaps not even then.
Moreover, in a high percentage of cases some pitfalls are only revealed after the damage is already done.
Let us simplify with an example; when a patient has a third molar with roots that are contiguous with the mandibular canal, we begin by trying to understand:
• whether the apices are separated from the nerve by a cortical layer or not;
• if the canal is spatially in a medial, lateral or central position;
• if a sonic handpiece osteotomy is preferable to a rotary one;
• where to perform the osteotomy and/or any dissection of the tooth;
• how not to damage the second molar with the previous dissection procedures;
• which side luxation and avulsion levers should be used to eliminate risk;
• the level of risk, so that a decision to proceed with the case or refer it can be made;
• how to draw up proper, respectful informed consent for the patient to avoid any disputes;
• how to quantify the value of our work in relation to the risk and time involved.
These considerations should be extended to:
• teeth that have apexes that are contiguous with the floor of the maxillary sinus;
• teeth that have periradicular rarefactions hidden by the roots themselves;
• endodontic or periodontal lesions involving the Schneiderian membrane;
• retained teeth requiring extraction or orthodontic anchoring;
• assessment of thin or absent cortical structures as a decisive parameter in cases of crowding for the extraction/non-extraction of one or more teeth.
In fact, the number of cases for which 3D data is needed is increasing as our knowledge expands.
Let us consider a case of complete edentulism in a very young patient, but without teeth for more than 20 years. This treatment is to be finalized via 8 implants, positioned with a software-assisted surgical guide using a non-flapless approach.
The Cone Beam 3D exam was acquired using the NewTom GiANO HR Professional and a 13 x 10 cm FOV (Field Of View, or volume size).
The great leap occurs mentally in the moment we are able to "look at" the patient, already imagining him/her in 3D. That is, imagining the effects of centripetal resorption of the upper jaw, the reduction of volumetric size referred to the correct spatial planes (coronal-apical in fig. 6-8 and bucco-palatal in fig. 9), yet with the awareness that we are unable to imagine the density of the medullary component, which will strongly impact the scope for immediate implantation.

Fig. 6 Details of the pre-molar area, upper right semi-arch

Fig. 7 Detail of the medial incisive canal in area 21

Fig. 8 Details of the upper left semi-arch molar

Fig. 9 Series of panoramic slices, 1 mm thick
With this new mindset we can choose "how to investigate" and how to help the patient face a moment that almost always causes anxiety; it also leads to higher level of attention when assessing the degree of safety with respect to the specific case.
Of course, a volumetric examination cannot, on its own, solve neither a simple nor a complex case. It needs to be performed correctly. It is necessary to have a machine with an exposure that has little interpolation (i.e. one that makes a complete orbit of the skull, emitting a spot for each degree of rotation, not the one that goes from 360° to 200° or little more, "inventing" what was not acquired as information), a machine with a high quality sensor that does not require image processing software to improve the iconography. The ideal machine would be the one of sufficient quality to provide a complete RAW Dataset, thus providing the "truth" with respect to what might be a more appealing image that, however, has been post-processed to make it so.
It should also be the one that does not resort to stitching to create a complete volume. It should be one in which the X-ray dose is calculated automatically and not left to the user's initiative, one that makes it easy to use the data. Whether choosing which centre to refer a patient to for the examination or choosing the right machine to buy, the assistance of honest professionals - who can provide key information in the appropriate format, persons not just motivated by making a sale of their "product" - is a must. The higher level of awareness that stems from familiarity with this 3D data also improves our critical thinking skills when we consider clinical approaches, scientific papers and, indeed, culture in general.
Conclusions
A technology that has an incredibly sophisticated hardware and yet is extremely user-friendly constitutes an optimal educational tool as long as, of course, one is willing to accept a learning curve that ultimately depends on our personal determination to better ourselves. To sum up: what happens when you start using volumetric data is that "fast" instinctive thought processes - to which we are accustomed, and which is based on an alteration of data that comes from a complete lack of information about one of the three planes making up a volume - changes and becomes a "slow" rational thought processes.
The authors of the work:
Daniele Benedetti Forastieri: Studio Dentistico Benedetti Forastieri-Guarrella (Senigallia)
Daniele Godi: Digital Workflow Expert at Revello S.p.A. (Verona)
With the impartial contribution of NewTom
For information: NewTom
 Related articles
Related articles

New initiative invites dentists to experience DEXIS’ most advanced AI yet, built on scale, speed, and clinical trust.
Products 04 June 2026

Recognized for its ergonomic, clinician-centered design that supports easy and comfortable integration of connected, cloud-based workflows into everyday clinical practice.

The cara Print Cube features a build area that can accommodate up to 5 full dental models, increasing throughput for dental professionals and lab technicians.
Products 02 June 2026
ETNA Rotary Instruments From Komet USA Well Suited for Zirconia and Ceramic Restorations

ETNA rotary instruments is a high-performance system of abrasive stones and 2-step polishers designed for zirconia and ceramic restorations.

The use of implant-retained overdentures has become an established standard of care for the edentulous arch, offering improved function, stability, and patient satisfaction compare
Read more
New initiative invites dentists to experience DEXIS’ most advanced AI yet, built on scale, speed, and clinical trust.
News 05 June 2026

(Nasdaq: ALGN), a leading global medical device company that designs, manufactures, and sells the Invisalign® System of clear aligners, iTero™ intraoral scanners, and exocad™ CAD/C
News 05 June 2026

(Nasdaq: HSIC), the world’s largest provider of health care solutions to office-based dental and medical practitioners, today announced that its Board of Directors has elected Will

As the University of Colorado School of Dental Medicine celebrates the graduating DDS Class of 2025, we are proud to recognize the students and faculty members whose exceptional de
Oral surgery 05 June 2026

This peer-reviewed oral surgery article summarizes clinical evidence from International journal of oral and maxillofacial surgery (2026). It focuses on findings that may help dental professionals...



Copyright © 2026 - All Rights Reserved
ISSN 2767-1178