

Orthodontic-surgical treatment of a severe class II skeletal malocclusion: a case report
Authors: Alessio Casimiro, Francesco Gallo, Francesco Zingari, Simone Ghezzi, Eleonora Carozzi
Patients presenting a reduction of the lower third of the face (short face), associated with a severe deep-bite, often benefit from minimal pre-surgical orthodontic preparation directed at arch alignment without the leveling of the Spee curve of the mandibular arch (tripodization)[1]. In fact, in this way, the inferior incisors (which are not intruded beforehand) create a slide plane that allows the mandible to disclose the posterior sectors more during the surgical advancement.
In the postoperative period, it will be necessary to manage the inter-arch space that will be created between the molars, by means of the extrusion that will allow the molars themselves to come into contact and thus stabilize the post-operative mandibular position.
DIAGNOSIS AND ETIOLOGY
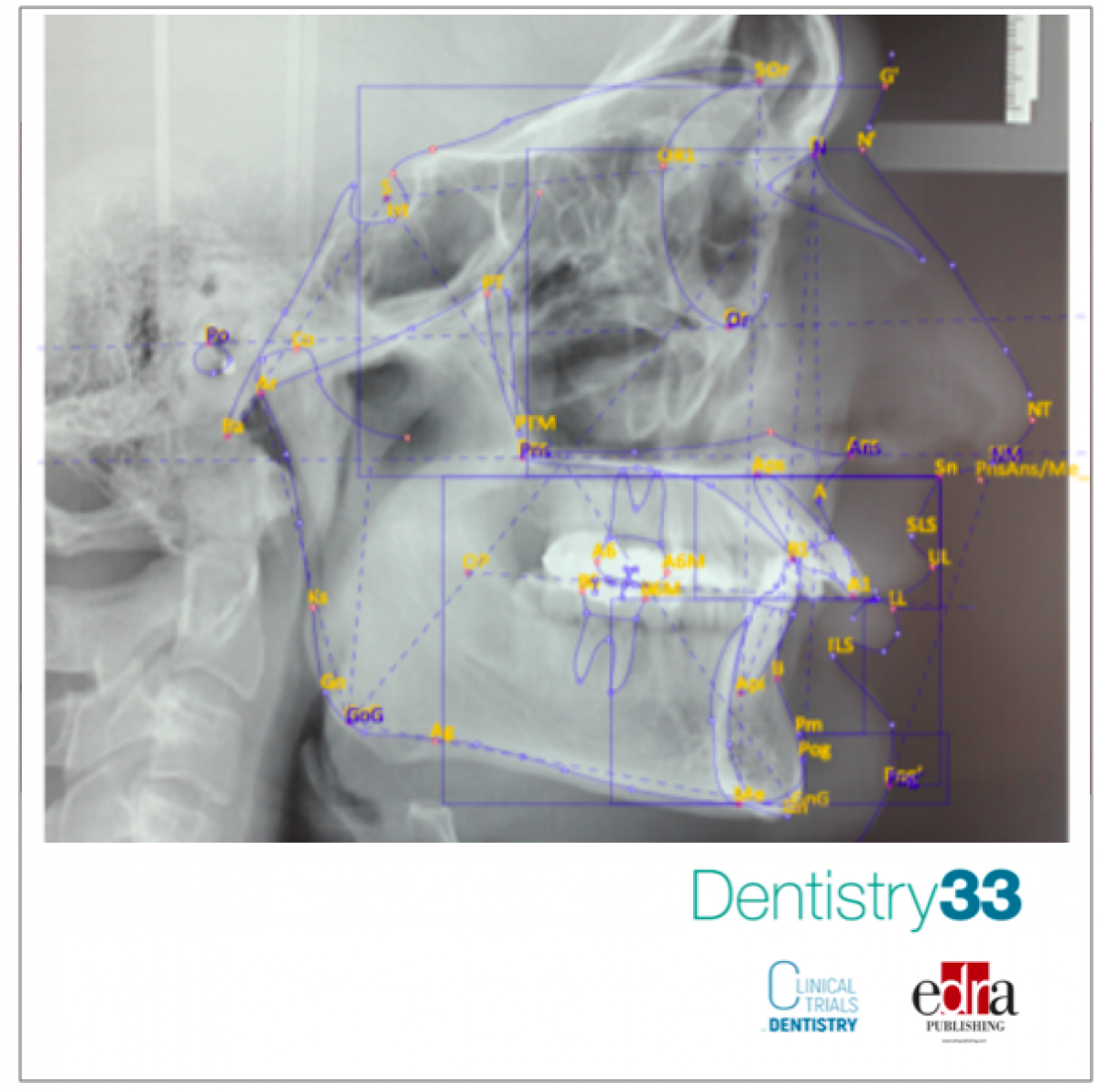
A young 26-year-old male patient came to our clinic (Clinica Briantea Odontostomatologica - CBO, Albiate - MB) with a request to improve his smile. From an anamnestic point of view, the patient did not present any contraindication to the treatment. The clinical and radiographic examination showed a picture of severe second skeletal class, convex profile, severe mandibular retrusion (ANB angle: 5°), hypodivergence (A. Intermax angle: 11°), skeletal deep-bite, excessive buccal-inclination of the upper incisors (I+/SN angle: 122°), everted lower lip, deep labial-mental sulcus, good representation of the skeletal symphysis, poor representation of the cervical-mental angle. (Fig. 1).
From the dental point of view, there was heavy attrition between the lower incisors and the palatal cingulum of the upper incisors, absence of the third molars, and of the element 2.6.
The dental arches showed moderate crowding. Increased overjet and overbite completed the malocclusion scenario. An objective examination of the temporomandibular joints did not reveal any signs of condylar-meniscal incoordination. The patient had no skeletal asymmetries.

Figure 1: Radiographic exams before treatment
TREATMENT OBJECTIVES
Harmonizing the patient's facial aesthetics by obtaining the first-class molar and canine occlusion, with reduction of the overjet and overbite, was the main goal of the treatment. The aims to be achieved for the improvement of facial harmony passed through the reduction of the facial convexity, the improvement of the chin projection, the reduction of the labio-mental sulcus, and the increase of the height of the lower third of the face. From the dental point of view, the alignment and coordination of the arches should have led to the complete correction of the second class canine/molar relationship, the reduction of buccal corridors, the improvement of incisal exposure, and the correction of excessive overjet and overbite.
TREATMENT ALTERNATIVES
After having discussed with the patient the non-surgical alternative, which would have provided an orthodontic therapy of "camouflage" of the second dento-skeletal class (extraction of the first upper premolars in order to reduce the overjet, leveling of the lower arch with the aid of TADs to reduce the overbite), the patient opted for the combined solution in order to achieve an improvement in occlusion associated with the harmonization of skeletal relationships.
TREATMENT
The non-extractive orthodontic therapy was preceded by a phase of rapid, surgically assisted palatal expansion (SARPE) in order to adapt the inter-canine and inter-molar diameter to the future mandibular advancement. Six months after the palatal disjunction, the arches were bandaged using the MBT® multi-bracket system (slot 0.22x0.28). The alignment and decompensation phase of the dental arches, which lasted circa 12 months, did not include the leveling of the Spee curve of the mandibular arch by the selective intrusion of the lower incisors, in order to maximize the increase in height of the lower third of the face during mandibular advancement ("tripodizing") (Fig. 2-3)
From a surgical point of view, in addition to the bilateral sagittal osteotomy for mandibular advancement, a Le Fort I in three fragments of the maxilla was performed, making possible the coordination of the upper to the lower arch and a general improvement of the incisal display. Through lowering and mild chin advancement genioplasty, further improvement in facial balance was achieved. Following surgery, the patient was stabilized with inter-arch guide elastics for one week. Leveling of the mandibular arch began following removal of the stabilizing surgical splint. Leveling of the lower dental arch began immediately using elastics that were connected from the mandibular molars and premolars to two zygomatic mini-plates previously inserted during surgery. This allowed a rapid leveling of the mandibular occlusal plane. The detailed occlusion phase lasted 6 months, at the end of which the patient underwent debonding. The patient then underwent a period of containment, by means of a Hawley retainer for the maxillary arch and a retainer bonded in the lower arch in the inter-canal sector, and an accurate follow-up aimed at stabilizing the orthodontic and surgical result. The detailing occlusion phase lasted 6 months, at the end of which the patient underwent debonding. The patient then underwent a period of containment, by means of a Hawley retainer for the maxillary arch and a retainer bonded in the lower arch in the inter-canal sector, and an accurate follow-up aimed at stabilizing the orthodontic and surgical result.
RESULTS
Normalization of skeletal and dental relationships led to a dramatic improvement in facial aesthetics. Sagittal and vertical discrepancies were resolved thanks to mandibular advancement guided by the concept of "tripodizing" the occlusion. The labio-mental sulcus was dramatically reduced and the projection of the chin was subsequently normalized. The final aesthetics of the smile was improved by increased exposure of the incisors and a reduction in buccal corridors. Normalization of the overbite and overjet was achieved, resulting in precise intercuspation of the dental arches that presented a right and left molar and canine I class. The post-treatment OPT (fig.2) shows the parallelism of the dental roots, the condylar morphology, and the osteosynthesis means used during the fixation of the skeletal segments. Also clearly evident are the mini-plates used as a means of temporary anchorage for leveling the lower arch. Cephalometric overlap (Fig. 3) between pre-and post-treatment skull teleradiography shows substantial forward and downward advancement of the mandible and maxilla.

Fig. 2: Post-treatment OPT

Fig. 3: Cephalometric overlap
DISCUSSION
Unfortunately, the scientific literature does not have many articles concerning the concept of "tripodizing" the occlusion as a guide to mandibular advancement and consequent increase in facial height. In the specific case, it was decided to undertake this therapeutic option to maximize the vertical increase of the lower third of the face and minimize maxillary down-grafting (a procedure subject to high risk of post-surgical recurrence).
How much does tripod advancement of the mandible affect vertical facial gain? As much as it avoids selective incisor intrusion preoperatively. In a systematic review, from 2005, the amount of mandibular incisor intrusion during orthodontic treatment was within a range (-0.19mm to 2.84 mm) that varied depending on the type of equipment used [2]. Post-surgical leveling of the Spee curve using traditional mechanics and/or skeletal anchors (TADs and/or mini-plates) has also been shown to be a relatively stable long-term procedure [3]. Genioplasty is definitely the surgical procedure that helps to complete the height gain of the lower third of the face. As pointed out by Wessberg et al [4], in severe brachyphofacial patients, the deformity is often located in the anterior portion of the mandible. In fact, in the patient of the following report, the chin was displaced downward and forward, allowing the reduction of the labio-mental sulcus and increasing the height of the lower third of the face.
CONCLUSIONS
Orthodontic-surgical treatment of a patient with skeletal class II dysgnathia from mandibular sagittal hypo-development and reduced vertical facial height (short face) often requires non extractive orthodontic treatment, mandibular advancement, and often genioplasty. Leveling of the lower arch can also be performed after surgery (tripod mandibular advancement) as this procedure promotes vertical development of the lower third of the face.
Bibliography
1. Jacobs J., Sinclair P. “Principles of orthodontic mechanics in orthognathic surgery cases”. Am J Orthod. 1983; 84: 399-407.
2. Ng J., Major P., HeoG., Flores-Mir C. “True incisor intrusion attained during orthodontic treatment: a systematic review and meta-analysis”. Am J Orthod Dentofacial Orthop 2005; 128:212-9
3. De Praeter j., Dermaut L., Martens G., Kuijpers-Jagtman AM. “Long-term stability of the leveling of the curve of Spee” . Am J Orthod Dentofacial Orthop 2000; 121:266-72
4. Wessberg G., Fish L., Epker B. “The short face patient: surgical-orthodontic treatment options”.J. Clin. Orthod. 1982; 16:668-85
 Related articles
Related articles
Digital Dentistry 20 April 2026

To report a fully digital and guided immediate-load All-on-4 protocol conducted in Brazil on a 59-year-old male patient with an edentulous maxilla and a history of oropharyngeal cancer surgery,...
Endodontics 13 January 2026
Regenerative endodontic treatment has provided a treatment option that aims to allow root maturation.
Oral surgery 22 December 2025

A very uncommon kind of ameloblastoma that combines a traditional follicular or plexiform subtype with solid-type ameloblastoma and desmoplastic features is emerging as a distinct entity.
Endodontics 05 October 2025

Regenerative endodontic procedures (REPs) associated with apical surgery could represent an alternative treatment strategy for patients whose teeth present incomplete root formation and extensive...
News 28 August 2025

Smartee Denti-Technology announces the publication of a case report on the application of the S8-SGTB clear aligner therapy for treating adult Class II malocclusion in the Journal of Aligner...
Read more
Edra Professional Books 06 June 2026
Understanding Dental Insurance: A Practical Reference for Dental Professionals

Understanding Dental Insurance is an Edra professional dentistry reference focused on clinical practice, education and treatment planning.

New initiative invites dentists to experience DEXIS’ most advanced AI yet, built on scale, speed, and clinical trust.
News 05 June 2026

(Nasdaq: ALGN), a leading global medical device company that designs, manufactures, and sells the Invisalign® System of clear aligners, iTero™ intraoral scanners, and exocad™ CAD/C
News 05 June 2026

(Nasdaq: HSIC), the world’s largest provider of health care solutions to office-based dental and medical practitioners, today announced that its Board of Directors has elected Will

As the University of Colorado School of Dental Medicine celebrates the graduating DDS Class of 2025, we are proud to recognize the students and faculty members whose exceptional de



Copyright © 2026 - All Rights Reserved
ISSN 2767-1178